

What does it mean to be well?
What does it mean to be well?
A meditation on sickness and health.

On this day two years ago, my doctor entered the hospital room where I had already spent five days and nights under her care. We had been waiting for test results.

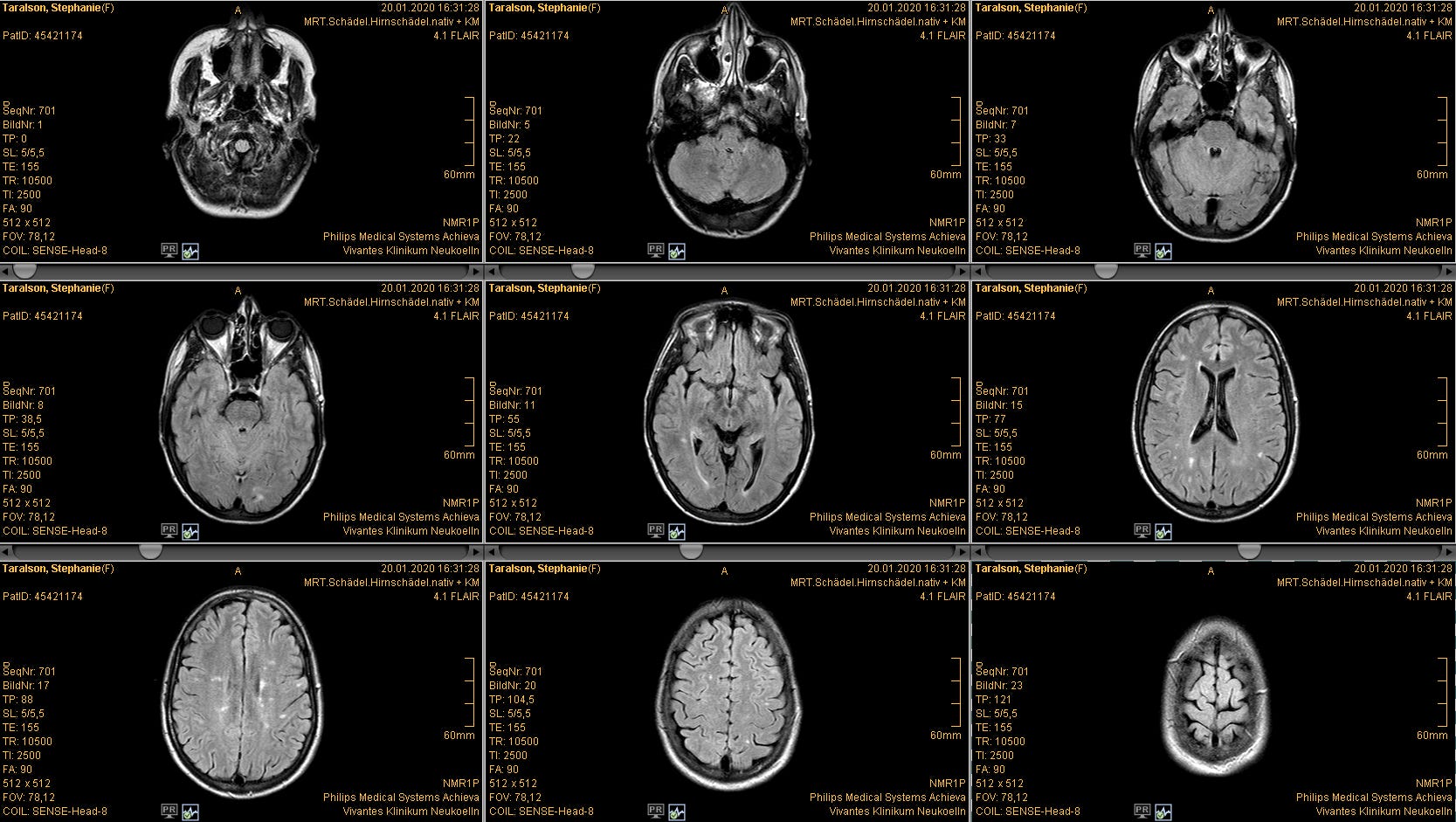
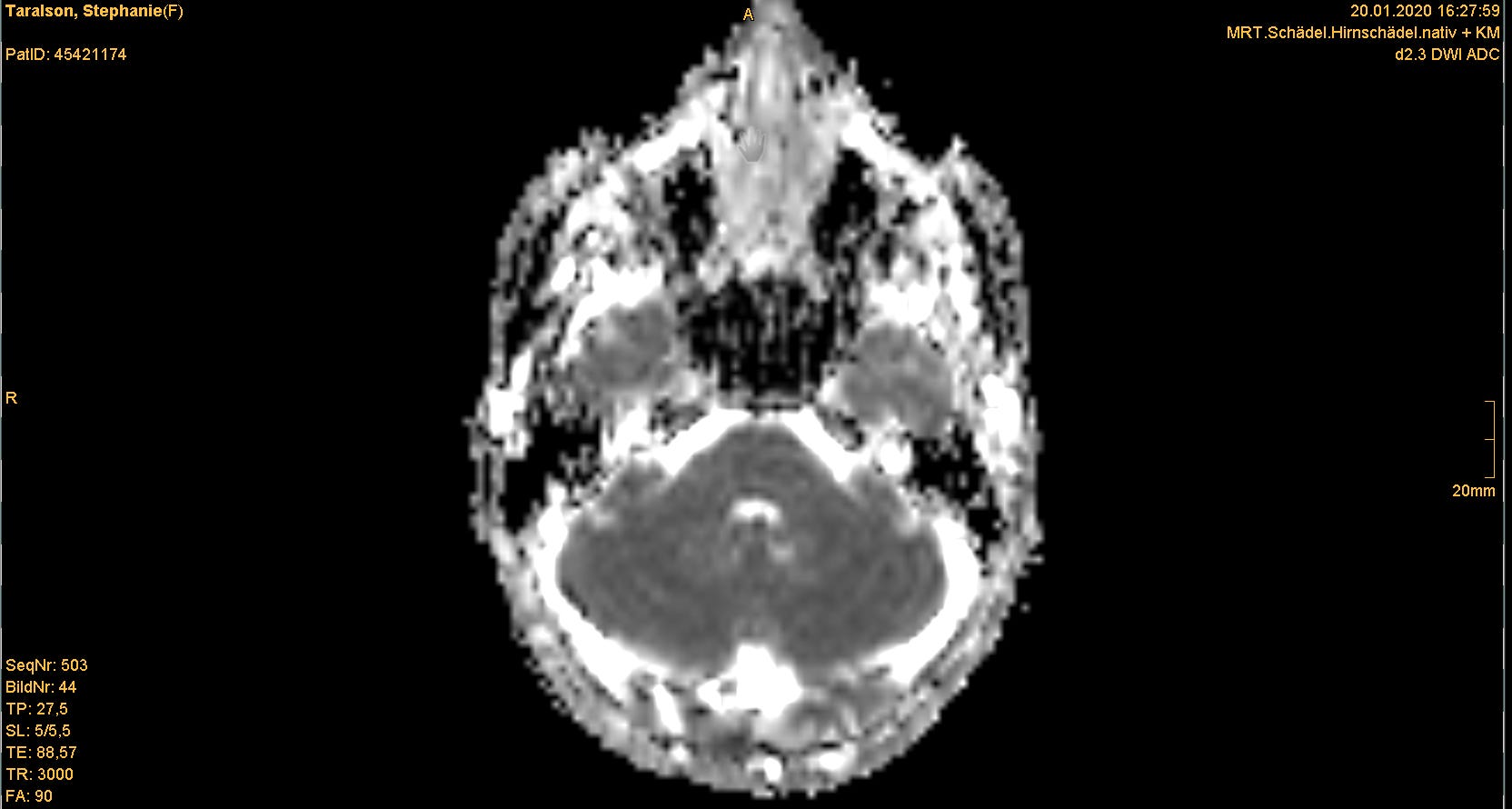
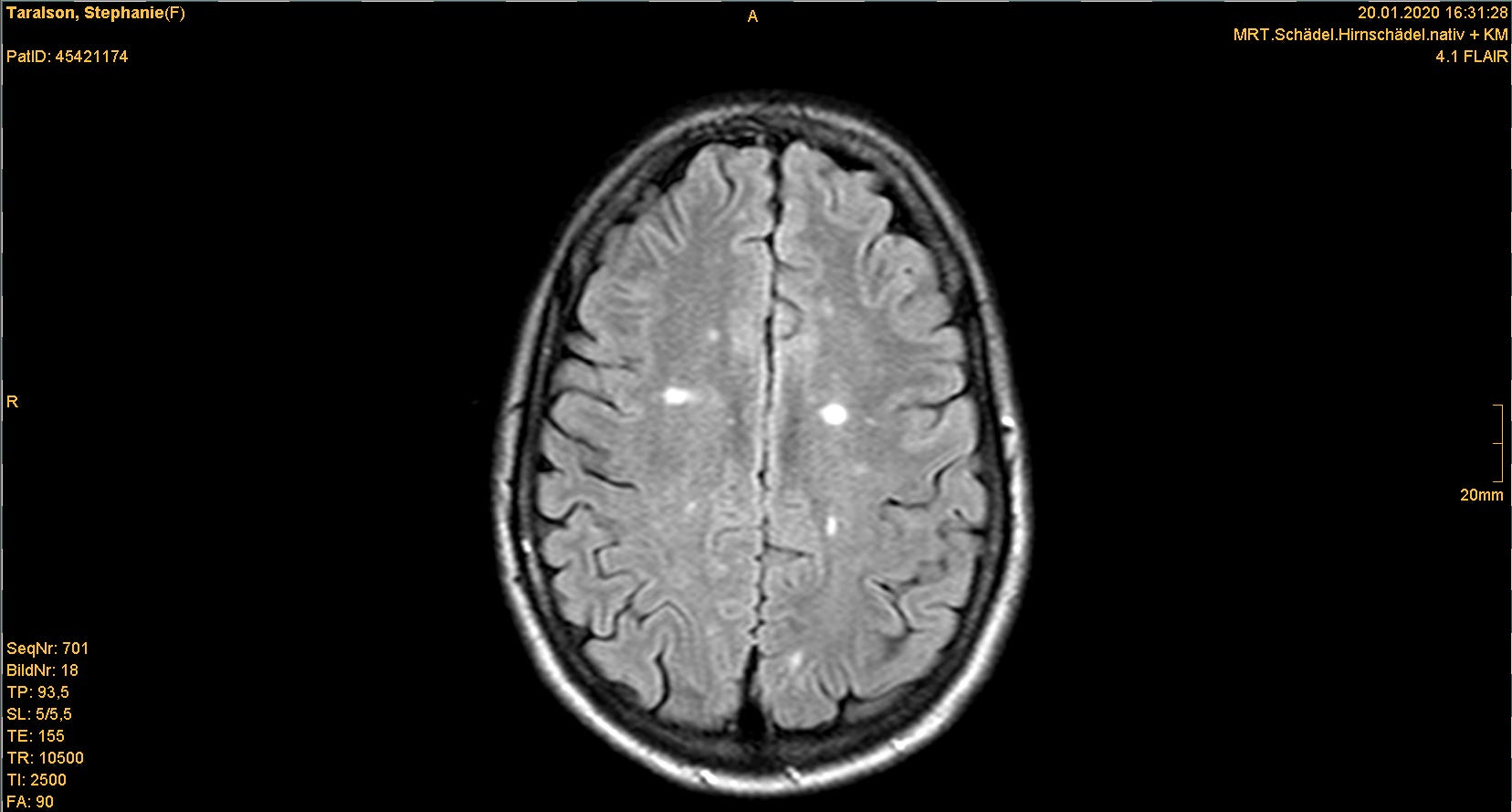
Dr. Meyer asked me to come with her to the office across the hall. It was a windowless room without any decoration or unnecessary furniture. The computers appeared to be running Windows 98. On-screen, Dr. Meyer clicked through dozens of photos from the MRI of my brain, showing me different cross-sections of this organ that is both the determinant and recipient of my human experience. Then, she told me that I have multiple sclerosis, a neurological autoimmune condition. It's degenerative and incurable.
The first tears came slowly but hot. I nodded at the doctor: "ich schaffe das."
I'll manage.
In retrospect, the MS diagnosis woefully undersold the scope and severity of what I would need to manage. Within six weeks of my discharge from hospital, the brokenness I perceived in having a self-harming body was externalized as other cornerstones of my life crumbled. My boyfriend broke up with me (saying he couldn’t imagine a shared future…not a particularly helpful thing to hear), a global pandemic broke out, and my workplace broke apart under the strain of said pandemic, leaving me jobless.
There was something cathartic about watching society collapse into anxiety and uncertainty in those first days of the pandemic, painfully similar to the uncertainty of my health. MS is characterized by unpredictability and is unique in every person who has it. Recovery from the episode that landed me in hospital was gradual and unsettled; I woke up every morning afraid to open my eyes, in case the symptoms that affected my sight were back.
The prospect that I could someday be well became a flickering possibility.
I wish I could say it got better right away. There’s evidence in my gratitude journal (I know, I know – but it really works) that I found things to celebrate and enjoy, even in those early months. But my first year was also a saga of failed treatment, disease progression, and repeated relapses. I went to the neurology clinic almost as often as I went to one of those desperate Zoom happy hours. To help cope with the depression and anxiety, I searched at length for a therapist that my health insurance would cover. A new romantic relationship was a frantic distraction; it was ill-fated and short-lived. My weight plummeted due to stress and disordered eating. The pandemic continued into a second wave.
It sounds contrived to say that I can pinpoint the exact moment when things started to get better. Even more clichéd: it was the first moment of January 1, 2021. I was in rural Canada, alone on the porch with sparkling wine in hand. Everything was snowed under, quiet, as the year turned. A Pandora’s box had been gaping open and finally, the lid clicked closed. 2020 is finished, I thought. It can’t hurt me anymore. 2021 was waiting, poised with its own cohort of struggles and hurts, and I recognized how arbitrary the new-year-fresh-start narrative was. I didn’t care. The prospect that I could someday be well became a flickering possibility.
In late January I started psychotherapy, and in February, a new MS treatment. In September, I got the good news that the medication was working and the disease had stopped progressing.
We are disabled by our environments, not our bodies.
And now it’s January again. This week, eying the approach of the two-year anniversary of my multiple sclerosis diagnosis, I’ve been reflecting on my experience of chronic illness.
It shouldn’t take a chronic illness to give me permission to treat my body kindly. I wish that we were all more generous with ourselves and more upfront with others about our needs and limitations. Riddled as we are with anxiety about status, safety, and social acceptance, we too often equate needs with moral weakness. Only when those needs become commodified and re-mechanised by capitalism are they again socially acceptable (see: ‘self-care’). Haley Nahman refers to “the animating tension of our shifting wants, needs, and abilities” and how “modern self-improvement discourse bifurcates behaviors along […] moralizing lines.”
Lately, I’ve been voraciously learning about the diversity of human experience and the social model of disability, which, despite having been in use since the 1980s, is still far outweighed by the more typical medical model of disability. Per the medical model, all limitations and disabilities are located within the disabled person, problematizing their very bodies and identifying them as the source of the ‘wrongness’. The medical model says that a person in a wheelchair is disabled because they can’t walk or that an autistic person is impaired because they can’t read social cues. By that logic, I’m disabled because I can’t work full-time–I need extra time each day to care for my body with rest, good nutrition, and exercise.
The social model of disability places the problem where it belongs: in the social environment. It decouples the disability from the person experiencing it. (This framework is reflected in the preference among many disability activists for person-first language, e.g. “person with a disability”.) In this model, a person in a wheelchair experiences disability when there are no ramps available, the sidewalk is too narrow, or the terrain is too uneven. An autistic person experiences disability because their style of social communication is misunderstood and rejected by non-autistic people. I am disadvantaged by a society in which full-time work is expected, because it’s an unreasonable expectation of me. We are disabled by our environments, not our bodies.
If my body could speak, it would say that it had been speaking all along but was only now being heard.
There are many degrees of human experience between the poles of “healthy” and “sick.” Suleika Jaouad writes and speaks with profundity about her experience of managing leukemia in her early 20s, saying:
Once I learned to accept my body and its limitations, I actually did start to feel better. And in the end, I think that's the trick: to stop seeing our health as binary, between sick and healthy, well and unwell, whole and broken; to stop thinking that there's some beautiful, perfect state of wellness to strive for; and to quit living in a state of constant dissatisfaction until we reach it. Every single one of us will have our life interrupted, whether it's by the ripcord of a diagnosis or some other kind of heartbreak or trauma that brings us to the floor. We need to find ways to live in the in-between place, managing whatever body and mind we currently have.
In the body I currently have, I manage. I have deep gratitude for my body, its resilience, and the privilege I continue to experience in it.1 Being better attuned to my physical existence means that I’m more aware these days of how to monitor and respect my own needs. To put it in meditative, pseudo-spiritual terms: if my body could speak, it would say that it had been speaking all along but was only now being heard.
When I mention that I manage a health condition, people still say that they hope I “get better soon.” They don’t know that I’m in the in-between place. I will never get better, and still, I am well.
Questions to Ask when it snows.
I chose to focus here on my experience as a person with an invisible disability. Nevertheless, I am a white middle-class cis-woman with manageable physical impairment and easy access to free healthcare. The points I make above about disabling environments also apply to other bodies: BIPOC, working-class, trans, and queer people are similarly disempowered by hostile environments.